

Join Us!
Partner with IGMHI to request services, training, and other support, or join as an Affiliate to assist in our mission.
Explore
Our Approach
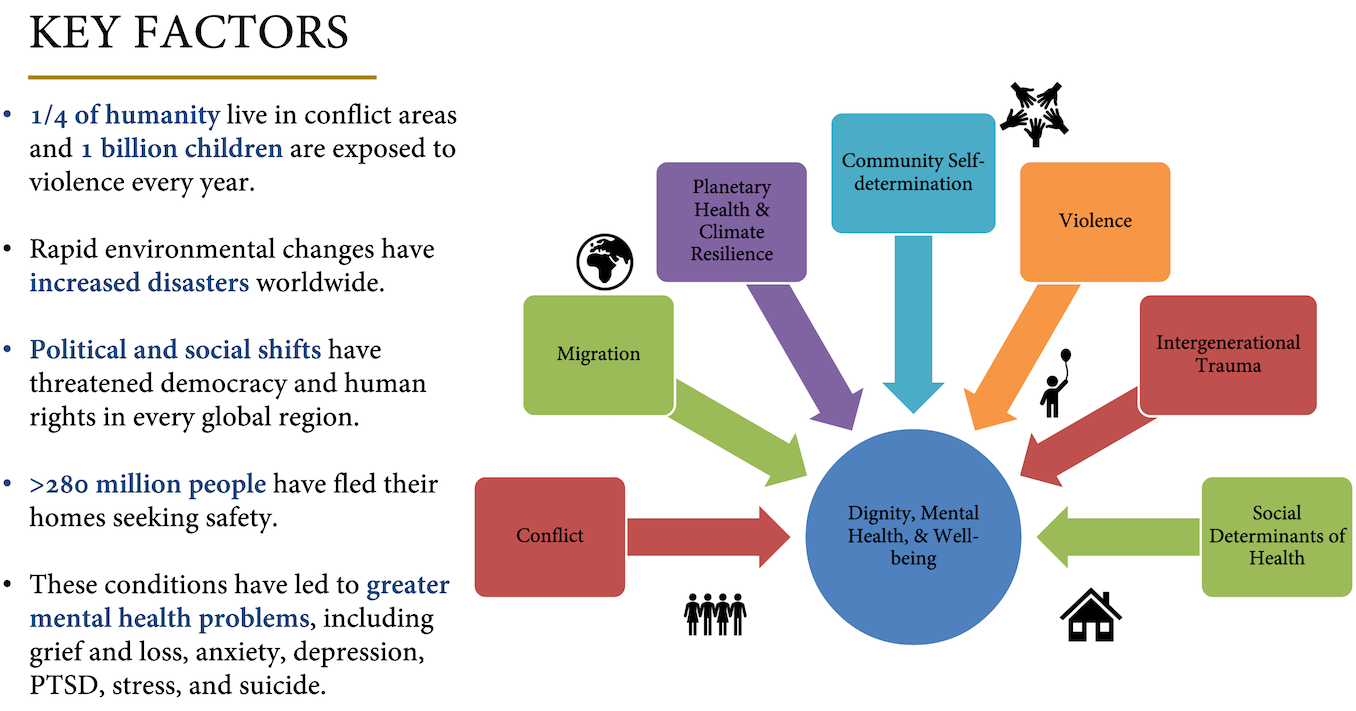
IGMHI provides community-engaged, culturally responsive, trauma-informed services to support resilience within communities around the world facing adversity and trauma related to climate change, armed conflict, crises, migration, human rights, and violence.
Learn MoreServices
IGMHI's provision of mental health care and support is grounded in evidence, applied research, cultural responsivity, community engagement, and sustainability. We offer education & training, technical assistance & capacity building, and mental health & psychosocial support.
Learn MoreInnovations
Our foundations of innovation promote connectedness both intersectorally and intergenerationally through communities, helping to enhance existing strengths, advance local workforce development, expand access to MHPSS services, reduce cultural barriers, and promote human rights.
Learn More
Help Support IGMHI
Donate to the Interdisciplinary Global Mental Health Innovation Fund today!


